

Letting the Storm Pass: The Psychology and Neuroscience of Mindfulness
Clement Doucette, Daniella Lorman, and Mara Russell
Illustrations by: Allie Verdesca

It’s the dead of winter, and you’ve decided that you need a break from the bitter cold of Upstate New York. As soon as you start driving south, a massive blizzard churns up, but it’s too late to turn back now. Shimmering flakes of white snow bombard your windshield, and you begin to feel dizzy and disoriented. The long strip of asphalt in front of you rapidly fades from view; no headlights can penetrate the raging squall that has engulfed your car. You decide to pull into the breakdown lane until the storm passes. Eventually, the snow settles, and the sun emerges and illuminates the road ahead, meaning you can continue your journey south. Like the maelstrom of a blizzard, practitioners of mindfulness argue that, by default, thoughts chaotically swirl through our minds. They believe that by practicing mindfulness, one can settle these chaotic thoughts and achieve personal clarity.
In the contemporary Western sense, mindfulness refers to a mental state in which an individual observes and focuses on their current thoughts, emotions, and inner experiences without judgement [1]. For over two thousand years, attaining this mental state has been integral to Buddhist religious practice. The teachings of Zen, which arose in seventh century China as a school of Buddhist thought especially professed the importance of breathing meditation in attaining self awareness [2]. Additionally, in the seventeenth century, teachers of Vipassana, a revived ancient Burmese Buddhist movement, instructed that spiritual insight could be attained through mindfulness meditation [3]. Mindfulness practices in psychotherapy were popularized and secularized in the Western world beginning in the 1960s and 1970s, as the general public became increasingly familiar with Zen Buddhist and East Asian spirituality and religious schools of thought.
DIFFERENT TYPES OF MINDFULNESS-BASED THERAPY
The development of the pioneering Mindfulness-Based Stress Reduction (MBSR) program by Dr. Jon Kabat-Zinn in 1979 sparked interest in potential medical applications of mindfulness activities. Inspired by both Zen Buddhist teachings and Vipassana practices, Kabat-Zinn developed MBSR to assist people with chronic pain, anxiety, depression, and stress. Individual components of MBSR include body scans, mindfulness meditation, and mindful breathing [4]. The body scan is a crisis survival technique that involves focusing on and accounting for each individual part of your body, from head to foot, and noticing how each part feels [5]. Similar to how laser copiers scan documents from top to bottom to record them, the body scans evaluates each portion of your body in order to center you in the present moment. Mindfulness meditation achieves a similar goal of centering oneself incorporating mindful breathing, which focuses on the motion’s of one’s breath, and exercises that compel the meditator to focus on different parts of their body [6].
DIALECTICAL BEHAVORIAL THERAPY (DBT)
MBSR practices influenced other schools of mindfulness-based therapy that emerged in subsequent decades. In the late 1980s, Dr. Marsha Linehan developed dialectical behavioral therapy (DBT) in an effort to treat symptoms of mood disorders, substance abuse, and suicidal ideation. Linehan developed the practice of radical acceptance, which aims to reduce suffering that arises from painful and traumatic experiences by interpreting and accepting present situations and emotions without judgement. If you simply experience, rather than repress or attempt to resist unpleasant emotions, Linehan argues that you will experience less anxiety and depression[7]. In a 24-week study conducted on 100 non-suicidal, non-self harming individuals, participants reported improved emotional regulation and better coping mechanisms, indicating that DBT may be beneficial for individuals with mood disorders [8].

MINDFULNESS-BASED COGNITIVE THERAPY (MBCT)
Mindfulness-based cognitive therapy (MBCT) is another psychotherapy approach that infuses traditional cognitive behavioral therapy (CBT) with mindfulness components. CBT aims to help people replace maladaptive coping mechanisms (such as isolating or substance abuse) with productive ones, changing the ways in which an individual reacts to stressful situations. CBT is commonly used to treat a myriad of disorders, including depression, substance abuse disorders, and obsessive compulsive disorder (OCD) [9]. MBCT takes these core practices of CBT and modifies them by introducing mindfulness practices. Integral and unique to MBCT, however, is the concept of decentering. The name itself is somewhat misleading; decentering oneself in MBCT involves being aware of and accepting incoming thoughts and feelings, but not judging or attaching oneself to them. Similar to radical acceptance, the individual remains centered in the present moment [10]. A common MBCT exercise involves eating a raisin and taking note of the various sensations you experience. For example, you may notice that parts of the raisin stick in your teeth, or how its sticky and wrinkled surface feels when the raisin rests on your tongue. By tuning in to your surroundings, you can learn to perceive subtle mental and physical sensations, equipping you with the tools to better address arising anxiety and discomfort [11].
This piece will discuss mindfulness practices as they impact psychological and neurological processes. Numerous studies have shown that mindfulness can lead to an increased tolerance of painful and uncomfortable situations, the reorganization of the brain, and an increased ability to engage in emotional processing.
MINDFULNESS AND PAIN
Everyone has felt the twinge of a pulled muscle, the sting of pricking yourself on a sharp object, or the pulsing throb of a headache. But have you ever wondered why we feel these miserable sensations? Pain, the perception of unpleasant sensations arising from a part of the body, teaches us to avoid harmful situations. When you stub your toe against a door or pull a muscle after a strenuous workout, your body and your brain work together to let you know that you have been hurt, prompting you to respond. Frequently, responding entails removing yourself from the damaging situation or resting an injured body part so it can heal.
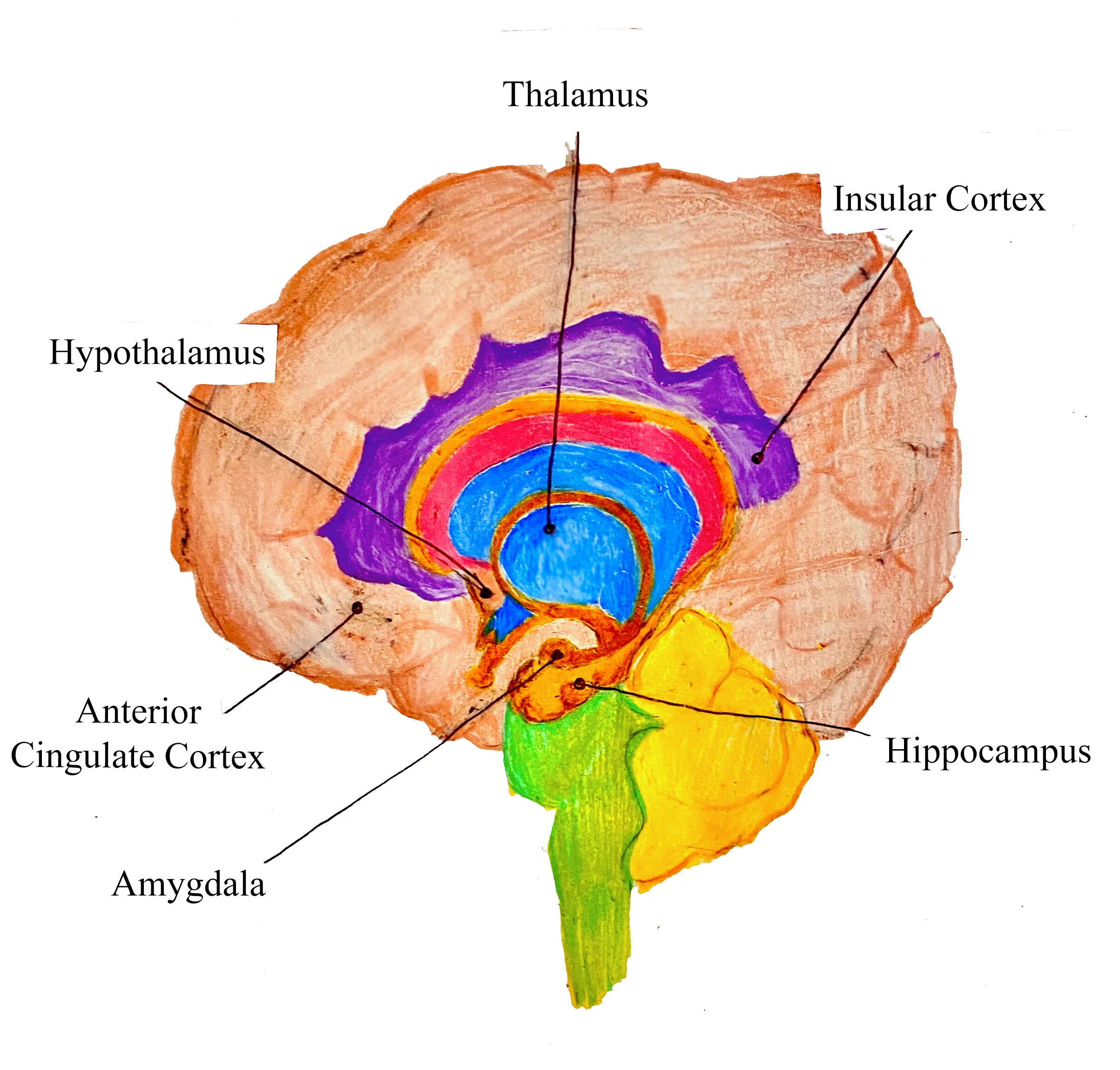
The sensory process that triggers the feeling of pain is called nociception. Free nerve endings, activated by a wide range of stimuli (extreme changes in temperature, oxygen deprivation, and mechanical force) that signal the damage of body tissue, are called nociceptors [12]. There are even specialized nociceptors that respond to selective stimuli; thermal nociceptors respond to scorching heat or extreme cold, while mechanical nociceptors respond to changes in pressure. In fact, most nociceptors are polymodal, meaning that they respond to a variety of categories of stimuli. When you prick your finger on a thumbtack, nociceptors transduce the painful stimulus into an electrical signal, which is sent up a bundle of nerves. These nerves synapse (or connect) onto your spinal cord, passing the signal up the spinal cord and to the brain. In the brain, the signals pass to the thalamus [13]. Think of the thalamus as the relay center of the brain; it processes and distinguishes between sensory stimuli, and directs input towards other brain regions which produce and remember feelings of pain (the amygdala and the hippocampus).
One important caveat of the standard pain pathway is that signals can be modified at several points. In 1965, Dr. Ronald Melzack and Patrick Wall proposed the Gate Control Theory of pain, suggesting that our spinal cord employs a “gate” mechanism, which opens to allow pain messages to reach the brain [13]. The Gate Control Theory proposes that pain signals can be amplified, blocked entirely, or slightly modulated, altering the perception of pain on a neurological level [13]. Recall an instance in which you were injured while being occupied with another task, perhaps during a sports game. It is likely that your perception of pain may have been diminished, as your brain decided to focus on the task at hand. In other words, your brain shut the “gate,” allowing you to pay attention to other messages.
There are two major categories of pain: chronic pain and acute pain [14]. Acute pain is a sudden, short-lived sensation that arises when you twist your ankle or step on a Lego. Following acute pain, sensory nerves carry the message of “ouch, that hurts” to your spinal cord, and then, your brain. Think of your brain as a database that stores knowledge of similar painful incidents in your life. Your brain files through previous painful situations, sorting through information to find a record of a similar type of injury, in order to decide an appropriate response. Sometimes, this response is a release of adrenaline or an increase in heart rate; other times, this response prompts you to remove yourself from the potentially damaging situation. Acute pain resolves once the injury is healed. On a neurological level, this means that nociceptors stop firing when the injury resolves [14]. Chronic pain is a long-lasting, persistent pain that lasts at least three months [14]. Individuals who experience chronic pain often have conditions that require long-term treatment and therapy to manage. One example of this is arthritis, a joint disease signaling disrepair. In contrast to acute pain, nociceptors in chronic pain continue to fire after the injury, resulting in a continued pain response even if there is no physical cause of pain present [14]. Chronic pain is a major health problem today, severely impacting the physical, social, and emotional functioning of individuals who suffer from it [15].
Now that we have explored the feeling of pain on a neurological level, it is important to note that response to pain is unique to the individual [16]. In other words, what may be slightly uncomfortable to one person may be excruciatingly painful to another. Because pain stimuli reach brain regions that process emotion, such as the amygdala, your experience of pain is shaped by emotional, social, and psychological factors. Your upbringing, social and cultural influences, beliefs and values, and previous pain memories are all contributory factors for interpreting pain [16]. For example, the pain response to stepping on a Lego will be different depending on the events preceding the accident: getting into an argument or celebrating an achievement will most likely result in differing pain perceptions and responses. In fact, your feelings about the experience may be impacted if your foot became infected the last time you stepped on a lego, perhaps hindering your rate of recovery. Because the causal factors of pain are multidimensional, the treatment of chronic pain is often challenging.
Recently, mindfulness in the form of meditation has been explored as an alternative for chronic pain patients seeking self-facilitated, drug-free therapy in an experimental setting [17.18,19]. While it remains unknown whether mindfulness meditation can directly intercept pain pathways, it has been found to alter activity in various brain regions and, in some cases, decrease sensitivity to pain [17,18,19]. One study required participants to focus attention on their breath while acknowledging any thoughts or emotions that arose without judgment, for just 20 minutes a day [17]. Participants showed a significant reduction in activity in the hippocampus— a brain region involved in processing the evaluation of pain— after just four days of practicing mindfulness mediation [17]. Another MBSR study that measured brain activity in long-term Zen meditation practitioners showed similar findings; participants showed a reduction of activity in their prefrontal and orbitofrontal cortices, two brain regions also active in processing the evaluation of pain [18]. The prefrontal cortex can be thought of as the control tower of your brain; it plays a cardinal role in higher-order decision making processes, focusing your attention, and in managing emotional reactions. The orbitofrontal cortex is an area of the prefrontal cortex that is involved in emotion and memory processing. In fact, the aforementioned study found that long-term Zen meditation practitioners exhibited increased activation in brain regions that process sensory (nociceptive) stimuli, such as the thalamus and the insula [18,19,20]. Additionally, mindfulness meditation has consistently been found to reduce chronic pain symptoms [21,19,22]. These findings suggest that individuals who practice mindfulness may experience increased feelings of control and reduced levels of anxiety when faced with painful situations.
MINDFULNESS AND NEUROPLASTICITY
Your brain is powerful and malleable. It has the ability to reorganize itself and change its structure over time. The technical term for this phenomenon is neuroplasticity. The human brain is composed of 100 billion neurons, or specialized cells that carry information throughout the body using electrical and chemical signaling processes. In the small pocket of space between two neurons, called the synapse, connections can form. In fact, the average adult brain is believed to have over 100 trillion neural connections [23]. Each time we learn something new, synaptic connections called neural pathways are “carved out” in the brain; your brain is constantly changing as new neural pathways are formed.
In 1949, Dr. Donald Hebb published neuroscience’s widely-used explanation of how learning is accomplished in the brain: Hebbian Theory, which says that neurons strengthen their neural connections by firing electrical impulses in sync [24]. However, these neural connections are not permanent [25]. Neuroscientist Dr. Carla Shatz suspected a fine-tuning mechanism in the brain, coining one of the best known aphorisms in neuroscience: “neurons that fire together wire together,” and its corollary “neurons that fire out of sync lose their link” [25]. As you practice or repeat learned skills, you maintain the neural pathway for that skill. This is akin to strengthening a new friendship. After befriending someone, hanging out and communicating are great ways to sustain your new relationship. However, if you never speak to your new friend, the relationship will fade. Shatz’s theory of neuroplasticity insinuates that the connections we sustain in our brain change as we age. The skills vital to your survival and functioning at age two are likely very different than those valuable to you today. Shatz’s theory postulates that pathways for skills that haven’t been used in a while get pruned away to make room for other, more useful connections; in other words, use it or lose it. Now that we have a handle on human brain plasticity, let’s explore mindfulness meditation’s ability to reorganize neural pathways and brain structure.
Several studies have surfaced with research supporting the claim that mindfulness meditation can lead to neurological changes. In one study, Western meditation practitioners were found to have increased thickness in cortical regions associated with sensory processing and attention [26]. Your cortex is the outermost part of your brain, primarily composed of grey matter, or neuronal cell bodies. As the largest site of neuronal integration (neurons receiving and transmitting information) in the brain, your cortex plays a critical role in attention, awareness, thought and memory-processing. As you age, your cortex thins out; however, different regions of the cortex have different susceptibility to aging, and therefore, thinning [27, 28]. The thinning of your cortex is correlated with a decrease in cortex-mediated processes, such as those aforementioned. Therefore, mindfulness practitioners with increased cortical thickness in distinct regions are more likely to retain sustained regulation of cortex-mediated processes than those who do not practice mindfulness. In other words, individuals who practice mindfulness may have increased attention and thought-processing ability. Another study found that after eight weeks of mindfulness meditation, participants’ amygdala size shrunk compared to those who were not practicing mindfulness, correlating with a decrease in stress [29].
MINDFULNESS AND EMOTIONAL REGULATION
Emotions are short-lived and defined states of positive or negative reactions to stimuli or situations [12]. There are three main components of emotion: physiological, behavioral, and cognitive. Imagine someone about to give an important presentation. Their palms are sweaty, their heart starts to race, their breathing becomes shallower. These are physiological responses. Sitting in their chair, they bounce their leg up and down, open their eyes wider, and twirl a pencil in their fingers. These are behavioral responses. Thinking to themselves, they remark, “I am so anxious, I just want this presentation to be over!” This is a cognitive appraisal of the emotion: anxiety.
There is much debate in the field of neurophysiology about how emotions are actually processed. However, most scientists agree that a network known as the limbic system, a loose collection of structures surrounding the thalamus, is responsible for emotion generation. Once generated by the limbic system, emotional information must be processed, and behavioral responses, regulated. This emotional regulation in the brain can be broken into two components: explicit and implicit regulation. Implicit regulation includes all the automatic and unconscious processes of emotion. Areas like the anterior cingulate cortex and medial (middle) prefrontal cortex are implicated in bottom-up regulation [31, 32]. Explicit regulation includes all the conscious and voluntary mental activity associated with emotional processing. In the brain, the central executive network (CEN) is usually involved in this explicit regulation. Although scientists define the regions included in the CEN differently, most agree that it includes the lateral (side) prefrontal cortex, and posterior (back) parietal cortex [20, 31, 32]. Simply put, when the brain regulates emotion, explicit regulation regions in the prefrontal cortex, such as the amygdala, control systems that generate emotions [31]. Implicit regulation areas work with emotion-generative areas to help inform the top-down system.
Now, just for a moment, take a break for yourself. Notice your emotions. What are you feeling? Confusion? Sadness? Joy? Hunger? As you sit with these feelings, simply observe them, without judgement. Try to name these emotions. What you have just performed is a common mindfulness task known as affect labelling. This and other mindful tasks have been linked to neural activation in key areas for emotional regulation [20]. Tasks like affect labeling affect the top-down system by simultaneously increasing activation in the prefrontal cortex and decreasing activation in the amygdala. This activation pattern suggests the prefrontal cortex regulates negative emotional responses like anger and fear. After and while performing an affect labeling task, several fMRI studies have demonstrated increased activation in areas of the prefrontal cortex, with a simultaneous decrease in amygdala activation [20, 32]. The increased activation of the prefrontal cortex leads researchers to believe that more emotional regulation is occurring [20].
Imagine a toddler who drops his ice cream cone on the ground. The subsequent responses are screams and tears: a temper tantrum. Young children, without a developed prefrontal cortex, have poor emotional regulation, especially in regulating negative emotions like sadness, anger, or fear. As a result, they have exaggerated emotional reactions to minute stimuli. Emotional regulation is a vital skill. In adults, many psychological disorders (such as depression, bipolar disorder, obsessive-compulsive disorder, and PTSD) are associated with reduced or dysfunctional emotional regulation [31]. Major depressive disorder, for example, is tied to higher levels of resting amygdala activity and lower prefrontal cortex activity compared to healthy subjects. Also, depressed patients demonstrate higher levels of amygdala reactivity to stimuli [33, 35]. However, studies comparing the neural correlates of mindfulness and depressive symptoms found great spatial overlap in the amygdala and medial prefrontal cortex, suggesting that practicing mindfulness could potentially alleviate symptoms of depression [34, 35]. An analysis of several studies found that while mindfulness was not as effective as medication and long-term therapy for mood disorders like depression and anxiety, mindful practices like meditation had a significant positive effect on relieving symptoms of those conditions [36].

THE DUALITY OF MINDFULNESS
Since the early 2000s, the frequency of the terms “mindfulness” and “meditation” in newspaper articles and scientific literature has increased exponentially [37]. However, delving into the findings of these studies presents a murky picture. Vague and inconsistently defined terminologies plague many of the articles. Significant methodological errors and small sample sizes render the data produced from several studies effectively meaningless. Furthermore, some of this literature suggests that mindfulness practices may be over-prescribed and even harm individuals by bringing repressed traumatic memories to light [37].
There is little consensus in the scientific community regarding the definition of mindfulness. Some adopt a definition referring to the regimen of meditative and centering practices included in MBSR therapy. Recently, others have considered mindfulness in much broader terms, interpreting it as the ability to be consciously aware of oneself and one’s feelings in the present moment [37]. These different definitions and practices of mindfulness may involve different regions of the brain and have different psychological effects. Even when using the same definition, empirical trials vary widely in the duration and intensity of mindfulness practice. In some studies, participants are “experts” at mindfulness; but, the level of practice required for such a title varies from paper to paper [37]. While one paper may utilize trained and practicing Buddhist meditators, others may define an expert as anyone who has done mindful exercises for only a few weeks.
FINAL THOUGHTS
While mindfulness, in all of its associated definitions, is an intriguing prospect with numerous exciting and potential clinical applications, it’s important to both recognize the flaws in existing research and acknowledge that more time is needed to uncover its biological and behavioral correlates. Fortunately, mindfulness is an easy skill to practice. Being mindful can simply entail carving out five minutes a day to tune in to your thoughts and feelings or complete a targeted exercise. Take a walk in the park without headphones in. Do a body scan. Download a mindfulness app to guide you. Regardless, if you find yourself stressed or fatigued, remember that relaxing your body may help to relax your mind.
REFERENCES
1. Hill, C.L.M., & Updegraff, J.A. (2012). Mindfulness and its relationship to emotional regulation. Emotion, 12(1), 81–90. https://psycnet.apa.org/doi/10.1037/a0026355
2. Singla, R. (2011). Origins of mindfulness & meditation interplay of Eastern & Western psychology. Psyke & Logos, 32(1), 220–239. https://tidsskrift.dk/psyke/article/view/8802
3. McMahan, D. L. (2009). The Making of Buddhist Modernism. New York, NY: Oxford University Press.
4. Kabat‐Zinn, J. (2003), Mindfulness‐based interventions in context: past, present, and future. Clinical Psychology: Science and Practice, 10: 144-156. https://doi.org/10.1093/clipsy.bpg016
5. Fischer, D., Messner, M., & Pollatos, O. (2017). Improvement of interoceptive processes after an 8-week body scan intervention. Frontiers in Human Neuroscience, 11. doi:10.3389/fnhum.2017.00452
6. Baer, R.A. (2003), Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology: Science and Practice, 10: 125-143. https://doi.org/10.1093/clipsy.bpg015
7. Linehan, M. (1993). Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: The Guilford Press.
8. Kells, M., Joyce, M., Flynn, D., Spillane, A., & Hayes, A. (2020). Dialectical behaviour therapy skills reconsidered: applying skills training to emotionally dysregulated individuals who do not engage in suicidal and self-harming behaviours. Borderline Personality Disorder and Emotion Dysregulation, 7, 3. https://doi.org/10.1186/s40479-020-0119-y
9. An, H., He, R., Zheng, Y., & Tao, R. (2017). Cognitive-behavioral therapy. Advances in Experimental Medicine and Biology Substance and Non-substance Addiction, 321-329. doi:10.1007/978-981-10-5562-1_16
10. Kuyken, W., Hayes, R., Barrett, B., Byng, R., Dalgleish, T., Kessler, D., … Byford, S. (2015). Effectiveness and cost-effectiveness of mindfulness-based cognitive therapy compared with maintenance antidepressant treatment in the prevention of depressive relapse or recurrence (PREVENT): A randomised controlled trial. The Lancet, 386(9988), 63–73. https://doi.org/10.1016/S0140-6736(14)62222-4
11. Felder, J.N., Dimidjian, S., & Segal, Z. (2012). Collaboration in mindfulness‐based cognitive therapy. J. Clin. Psychol., 68: 179-186. https://doi.org/10.1002/jclp.21832
12. Bear, M. F., Connors, B. W., & Paradiso, M. (2006). Neuroscience: Exploring the brain. Baltimore, MD: Lippincott Williams & Wilkins.
13. Garland, E. L. (2012). Pain processing in the human nervous system: a selective review of nociceptive and biobehavioral pathways. Primary care, 39(3), 561–571. https://doi.org/10.1016/j.pop.2012.06.013
14. Raffaeli, W., & Arnaudo, E. (2017). Pain as a disease: an overview. Journal of Pain Research, 10, 2003–2008. https://doi.org/10.2147/JPR.S138864
15. Veehof, M. M., Trompetter, H. R., Bohlmeijer, E. T., & Schreurs, K. M. G. (2016). Acceptance- and mindfulness-based interventions for the treatment of chronic pain: A meta-analytic review. Cognitive Behaviour Therapy, 45(1), 5–31. https://doi.org/10.1080/16506073.2015.1098724
16. Bekanich, S. J., Wanner, N., Junkins, S., Mahoney, K., Kahn, K. A., Berry, C. A., ... Gardner, A. J. (2014). A multifaceted initiative to improve clinician awareness of pain management disparities. American Journal of Medical Quality, 29(5), 388–396. https://doi.org/10.1177/1062860613503897
17. Zeidan, F., Emerson, N. M., Farris, S. R., Ray, J. N., Jung, Y., McHaffie, J. G., & Coghill, R. C. (2015). Mindfulness meditation-based pain relief employs different neural mechanisms than placebo and sham mindfulness meditation-induced analgesia. Journal of Neuroscience, 35(46), 15307–15325. https://doi.org/10.1523/JNEUROSCI.2542-15.2015
18. Zeidan, F., & Vago, D. R. (2016). Mindfulness meditation-based pain relief: a mechanistic account. Annals of the New York Academy of Sciences, 1373(1), 114–127. https://doi.org/10.1111/nyas.13153
19. Gard, T., Holzel, B. K., Sack, A. T., Hempel, H., Lazar, S. W., Vaitl, D., & Ott, U. (2012). Pain attenuation through mindfulness is associated with decreased cognitive control and increased sensory processing in the brain. Cerebral Cortex, 22(11), 2692–2702. https://doi.org/10.1093/cercor/bhr352
20. Hölzel, B. K., Carmody, J., Vangel, M., Congleton, C., Yerramsetti, S. M., Gard, T., & Lazar, S. W. (2011). Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Research: Neuroimaging, 191(1), 36–43. https://doi.org/10.1016/j.pscychresns.2010.08.006
21. Morone, N. E., Greco, C. M., & Weiner, D. K. (2008). Mindfulness meditation for the treatment of chronic low back pain in older adults: a randomized controlled pilot study. Pain, 134(3), 310–319. https://doi.org/10.1016/j.pain.2007.04.038
22. Lutz, A., McFarlin, D. R., Perlman, D. M., Salomons, T. V., & Davidson, R. J. (2013). Altered anterior insula activation during anticipation and experience of painful stimuli in expert meditators. NeuroImage, 64, 538–546. https://doi.org/10.1016/j.neuroimage.2012.09.030
23. Zimmer, C. (2011). 100 trillion connections: new efforts probe and map the brain's detailed architecture. Retrieved December 25, 2020, from https://www.scientificamerican.com/article/100-trillion-connections/
24. Abraham, W. C., Jones, O. D., & Glanzman, D. L. (2019). Is plasticity of synapses the mechanism of long-term memory storage?. NPJ science of learning, 4, 9. https://doi.org/10.1038/s41539-019-0048-y
25. Shatz C. J. (2009). MHC class I: an unexpected role in neuronal plasticity. Neuron, 64(1), 40–45. https://doi.org/10.1016/j.neuron.2009.09.044
26. Lazar, S. W., Kerr, C. E., Wasserman, R. H., Gray, J. R., Greve, D. N., Treadway, M. T., ... Fischl, B. (2005). Meditation experience is associated with increased cortical thickness: NeuroReport, 16(17), 1893–1897. https://doi.org/10.1097/01.wnr.0000186598.66243.19
27. Fjell, A. M., Grydeland, H., Krogsrud, S. K., Amlien, I., Rohani, D. A., Ferschmann, L., … Walhovd, K. B. (2015). Development and aging of cortical thickness correspond to genetic organization patterns. Proceedings of the National Academy of Sciences, 112(50), 15462–15467. https://doi.org/10.1073/pnas.1508831112
28. Hurtz, S., Woo, E., Kebets, V., Green, A. E., Zoumalan, C., Wang, B., … Apostolova, L. G. (2014). Age effects on cortical thickness in cognitively normal elderly individuals. Dementia and Geriatric Cognitive Disorders Extra, 4(2), 221–227. https://doi.org/10.1159/000362872
29. Hölzel, B. K., et al. (2010). Stress reduction correlates with structural changes in the amygdala. Social cognitive and affective neuroscience, 5(1), 11–17. https://doi.org/10.1093/scan/nsp034
30. Hölzel, B. K., Carmody, J., Evans, K. C., Hoge, E. A., Dusek, J. A., Morgan, L., … Lazar, S. W. (2010). Stress reduction correlates with structural changes in the amygdala. Social Cognitive and Affective Neuroscience, 5(1), 11–17. https://doi.org/10.1093/scan/nsp034
31. Guendelman, S., Medeiros, S., & Rampes, H. (2017). Mindfulness and emotion regulation: insights from neurobiological, psychological, and clinical studies. Frontiers in Psychology, 8, 220. https://doi.org/10.3389/fpsyg.2017.00220
32. Lutz, A., Jha, A. P., Dunne, J. D., & Saron, C. D. (2015). Investigating the phenomenological matrix of mindfulness-related practices from a neurocognitive perspective. The American Psychologist, 70(7), 632–658. https://doi.org/10.1037/a0039585
33. Burklund, L. J., Creswell, J. D., Irwin, M. R., & Lieberman, M. D. (2014). The common and distinct neural bases of affect labeling and reappraisal in healthy adults. Frontiers in Psychology, 5, 221. https://doi.org/10.3389/fpsyg.2014.00221
34. Quirk, G. J. & Beer, J.S. (2006). Prefrontal involvement in the regulation of emotion: convergence of rat and human studies. Current Opinion in Neurobiology, 16(6), 723-727, https://doi.org/10.1016/j.conb.2006.07.004
35. Way, B. M., Creswell, J. D., Eisenberger, N. I., & Lieberman, M. D. (2010). Dispositional mindfulness and depressive symptomatology: correlations with limbic and self-referential neural activity during rest. Emotion (Washington, D.C.), 10(1), 12–24. https://doi.org/10.1037/a0018312
36. Goyal, M., Singh, S., Sibinga, E. M. S., Gould, N. F., Rowland-Seymour, A., Sharma, R., … Haythornthwaite, J. A. (2014). Meditation programs for psychological stress and well-being: A systematic review and meta-analysis. JAMA Internal Medicine, 174(3), 357. https://doi.org/10.1001/jamainternmed.2013.13018
37. Van Dam, N. T., van Vugt, M. K., Vago, D. R., Schmalzl, L., Saron, C. D., Olendzki, A., … Meyer, D. E. (2018). Mind the hype: a critical evaluation and prescriptive agenda for research on mindfulness and meditation. Perspectives on Psychological Science, 13(1), 36–61. https://doi.org/10.1177/1745691617709589